
Newer Proposed Classification of Mandibular Fractures: A Critical Review with Recent Updates
Citation: Deepak Passi. Newer Proposed Classification of Mandibular Fractures: A Critical Review with Recent Updates. Ann Med Health Sci Res. 2017; 7: 314-318
This open-access article is distributed under the terms of the Creative Commons Attribution Non-Commercial License (CC BY-NC) (http://creativecommons.org/licenses/by-nc/4.0/), which permits reuse, distribution and reproduction of the article, provided that the original work is properly cited and the reuse is restricted to noncommercial purposes. For commercial reuse, contact reprints@pulsus.com
Abstract
In maxillofacial trauma, the mandible is the most common facial fracture after nasal bone. Mandible fractures are among the most common skeletal injuries in following trauma due to its anatomical location and less support from cranium. This vulnerable bone is an active mobile articulation with the maxillary dentition. For appropriate management of mandibular fracture, a comprehensive and therapy relevant classification is required. There are number of classifications quoted in medical literature with their merits and demerits. Fracture of mandible is classified by its anatomic location, condition, and position of teeth relative to the fracture, favorableness, or type, yet no classification system have included the total avulsion/disarticulation of mandible. The classification should be easy to use, contain all the aspects of fracture (clinical and radiolographic) and easily understandable by clinician of different specialty. Aim of this article is to shortly review various classification systems of mandibular fracture and to propose a new classification including rarest case of total avulsion /dislocation of mandible from maxillofacial skeleton
Keywords
Fracture; Avulsion; Classification; Mandible; Dentition
Introduction
Mandible is the largest and main bone of the lower part of the face. Anatomic parts of the mandible are the symphysis, parasymphysis, body, angle, ramus, coronoid process, condyle, and alveolus. Inherent weak sites of mandible which is liable to fracture includes angle of mandible (especially when third molar is impacted), the socket of the canine tooth (due to long root of canine bone amount is less), and the condylar neck. Mandible fractures in maxillofacial trauma occur more commonly due to prominence of mandible and comparative lack of bony and soft tissue support. Mandibular fracture is the 2nd most common fracture of the face after nose and 10th most common fractured bone in the human body. Forces required to produce a fracture of the mandible is about 70 – 100 g [1].
There are a lot of classifications of mandibular fractures in literature. Fracture of mandible has been classified according to anatomical Location, Type, Involvement of dentition, Displacement and Favorability of treatment but Total/ complete avulsion of mandible is not included or categorized in any classification. The most important requirement for the appropriate treatment of mandible fractures is an easy, well defined, unambiguous and therapy-relevant classification. So an attempt is being made here to revise a comprehensive classification of mandibular fractures which includes all the components of fracture along with inclusion of the particular case of total avulsion of mandible in this review.
Various classification systems of mandibular fracture as described in literature are enlisted below.
1. Dingman and Natvig
They classified mandibular fractures in several categories. This classification is mostly used in clinical practice [2].
• According to the direction of the fracture (Figure 1)

Figure 1: Horizontally favorable/unfavorable and vertically favorable/ unfavorable fractures.
1(a) Horizontally favorable
1(b) Horizontally Unfavorable
1(c) Vertically Favorable
1(d) Vertically Unfavorable
• According to the severity of the fracture
a) Simple
b) Closed
c) compound
d) Communited
• According to the type of fracture:
Greenstick fracture, Comminuted fracture, Complex fracture, depressed fracture, impacted fracture and Pathological fractures.
• According to the presence or absence of the teeth in the jaws:
a) Dentulous,
b) Partially edentulous,
c) Edentulous
•According to the location (Figure 2)
Symphysis, parasymphysis, body region, angle region, ramus region, condylar process, coronoid process

Figure 2: Classification of mandibular fracture according to anatomical location.
2. Kelly and Harrigan
Classified mandibular fractures into six categories for simplification in classification [3]
• Fracture of symphysis
• Fracture of body
• Fracture of angle
• Fracture of ramus
• Fracture of condylar process
• Fracture of coronoid process
3. Lindah and Hollender
Classification of mandibular condyle fracture [4].
• According to anatomical loaction
a) condylar head or intracapsular fracture
b) condylar neck
c) subcondylar region or extracapsular fracture
• According to degree of fracture fragment displacement
a) Non displacement
b) Deviation
c) Displacement
d) Deviation –dislocation
e) Displacement –dislocation
f) Lateral override
g) Medial override
4. Kazanjian and Converse
Dentition Classification of mandibular fracture [5]. (Figure 3)

Figure 3: mandibular fracture.
• Class I: Teeth are present on both sides of the fracture line
• Class II: Teeth are present only on one side of the fracture line
• Class III: Fracture in edentulous patient
5. Kabakov and Malishev
The most popular classification [6].
• According to localization:
Mandibular body/with or without teeth in fracture line
Mandibular ramus with its processes
• According to the character:
With dislocation
Without dislocation
• According to the number:
• Single, double, multiple, unilateral, bilateral
6. Kruger and Schilli
He took into account many of the aforementioned classifications described and developed four categories of mandibular fractures [7].
• Relation to the external environment : (a) Simple/closed, (b) Compound/ open
• Types of fractures: (a) Incomplete, (b) Greenstick, (c) Complete, (d) Comminuted
• Dentition of the jaw with reference to the use of splints
• Sufficiently dentulous jaw
• Edentulous or insufficiently dentulous jaw
• Primary and mixed dentition
• Localization
• Fractures of the symphysis region between the canines
• Fractures of the canine region
• Fractures of the body of the mandible between the canine and angle of the mandible
• Fractures of the angle of the mandible in the third molar region
• Fractures of the mandibular ramus between the angle of the mandible and sigmoid notch
• Fractures of the coronoid process
• Fractures of the condylar process
7. Sinn, Hill and Watson
Classification of fractures according to the anatomical locations similar to “E” of Dingman’s classification [8].
• Condylar fractures/intracapsular
• Subcondilar fractures
• Coronoidal fractures
• Fractures of mandibular ramus
• Fractures of mandibular angle/open through third molar socket
• Fractures of mandibular body/open through tooth socket
• Fractures of symphysis
8. Pogrel and Kaban
He classified mandibular fractures in 5 groups according to the site of injury [9].
• Condylar fractures
• Ramus fractures
• Angle fractures
• Body fracture
• Fractures of symphysis and parasymphysis
9. Gratz
He classified newer classification It consists of alpha-numeric system similar to TNM classification of tumours [10].
• F- Fractures
• L- Localization
• O- Occlusal disorders
• S- Soft tissues injuries
• A- Associated other maxillo-facial injuries
10. WHO
The international classification of mandibular fractures [11].
• S 02.6 - Fractura mandibulae
• S 02.60 - Fractura processus alveolaris
• S 02.61 - Fractura corpus mandibulae
• S 06.62 - Fractura processus articularis/condylaris
• S 06.63 - Fractura processus muscularis /coronoideus
• S 02.64 - Fractura ramus mandibulae
• S 02.65 - Fractura symphysis
• S 02.66 - Fractura angulus mandibulae
• S 02.67 - Fracturae mandibulae multiplex
• S 02.68 - Unspecified mandibular fractures
11. Pankratov and Robustova
They divided fracture into 8 categories with alphanumeric marks. These symbols characterize the line offracture, involved teeth, presence /or absence/ of dislocated fragments, occlusive disorders, combined injuries status of soft tissues, presence of inflammation in the fracture line and its severity [12].
• F-(Fracture): From Fo to F4 and includes: incomplete, simple, double and multiple fractures.
• T-(Tooth): To, T1, T2/T2 c, T2 pu, T2 pe, T2pa - includes information concerning tooth-periodontal or parodontal changes of tooth in the fracture line.
• L-( Localization): from L1to L8- and includes the following regions: L1 - incisivum, L2 - caninum, L3 -premolars – molars; L4 - angulus mandibulae L5 -ramus mandibulae; L6 - proc. condylaris; L7 - proc. muscularis /coronoideus/; L8 – proc. alveolaris
• O-(Occlusion): Oo, O1, O2 – with or without occlusal changes including classification of bone atrophyof the mandible/ O2-aI, O2-aII, O2-aIII; a I, II, III mark the bone atrophy of mandible.
• S-(Soft tissue): So-closed mandibular fracture, S1-open mandibular fracture /communication with oral cavity/, S2-open combined with skin injuries, S3-intra and extraoral opened fractures, S4- open fracture with soft tissue formations
• I-( Infection): Io, I1, I2 – with or without inflammatory changes/abscess and flegmonas
• A-(Associated): A0, A1 – combined or not.
12. Shetty et al.
He combined six significant injury criteria to create the acronym FLOSID, which essentially allowed for ease of assessment and defined fracture characteristics. They assessed mandibular fractures using the taxonomy described and added weighting factors to address severity [13].
• Fracture type (F): (a) Incomplete (b) Simple (c) Comminuted (d) Bone defect
• Location of fracture (L): (a) Left from midline (L1) to condylar head (L8) (b) Right from midline (R1) to condylar head (R8)
• Nature of occlusion (O): (a) Normal (b) Malocclusion (c) Edentulous
• Extent of soft tissue damage (S): (a) Closed (b) Open intraorally (c) Open extraorally (d) Open intra and extraorally (e) Soft tissue defect
• Presence of infection (I): (a) Yes (b) No
• Radiographic analysis of interfragmentary displacement (D): (a) Mild (b) Moderate (c) Severe
13. Etiologic classification
• Direct blow: Road Traffice Accident, physical assault, sport injury, Hit /Fall injury, industrial trauma (Figure 4)

Figure 4: Etiologic classification of mandibular fracture.
• Indirect blow
• Excessive muscle contraction: Fracture of coronoid process due to sudden reflex contracture of temporalis muscle.
Discussion
There exist a lot of classifications of mandibular fractures with their merits and demerits. Dingman and Natvig [2] classified Mandibular fractures into many division but not included occlusion, infection, dislocation component. Kelly and Harrigan [3] mandibular fractures were divided into six categories. It is similar to above classification but except the canine site was removed. Gratz [10] revised a common formula, and suggested digital alphabetical classification similar to tumors (TNM). It was the First attempt for unified and standard classification of mandibular fractures is known as formula of fracture of Gratz. This classification does not reveal any information such as dislocation of fracture and the teeth in fracture line. Pogrel and Kaban [9] classified mandibular fractures in five groups according to the location of the fracture. They mentioned only about the site of the fracture in their classification. WHO [11] given the international classification of mandibular fractures using unique numbers but demerit is that the last class “unspecified mandibular fractures” is not viable for clinical usefulness. Other important information like occlusion, presence of infection, tooth in the fracture line, soft tissue counterpart was not mentioned.
Pankratov and Robustova [12] proposed a classification which focuses on only clinical symptoms and does not contain the information that reflects the radiological considerations and also it is too lengthy. Schuknecht & Graetz proposed a radiographic classification. They use Spiral multislice CT to precisely quoting the mandibular fractures based on location, into alveolar, mandibular proper, and condylar fractures [14]. This classification can only be used where CT scan facilities are available. Shetty et al. [13] combined six significant injury criteria to create the acronym FLOSID, which essentially allowed for ease of assessment and defining fractures. They assessed mandibular fractures using the taxonomy described and added weighting factors to address severity. Buitrago-Téllez et al. evaluate a comprehensive classification system for mandibular fractures based on imaging analysis [15]. This system gives standard documentation of mandibular fractures, but clearity in sub categories and application status is still required.
So, it is necessary to point out that there is need of a classification which includes very well defined categories. These categories should be visualized radiologically and should be used easily by clinicians of different specialties. The classification of mandibular fractures should be easy for the routine work in Emergency and regular department. Also none of the present classification has included the total dislocation/avulsion of mandible in their classification like in mid-face classification of zygomaticocomplex (ZMC). Since the case has been reported [16] it should be included into classification. So an attempt is made here to revise the classification of mandibular fracture.
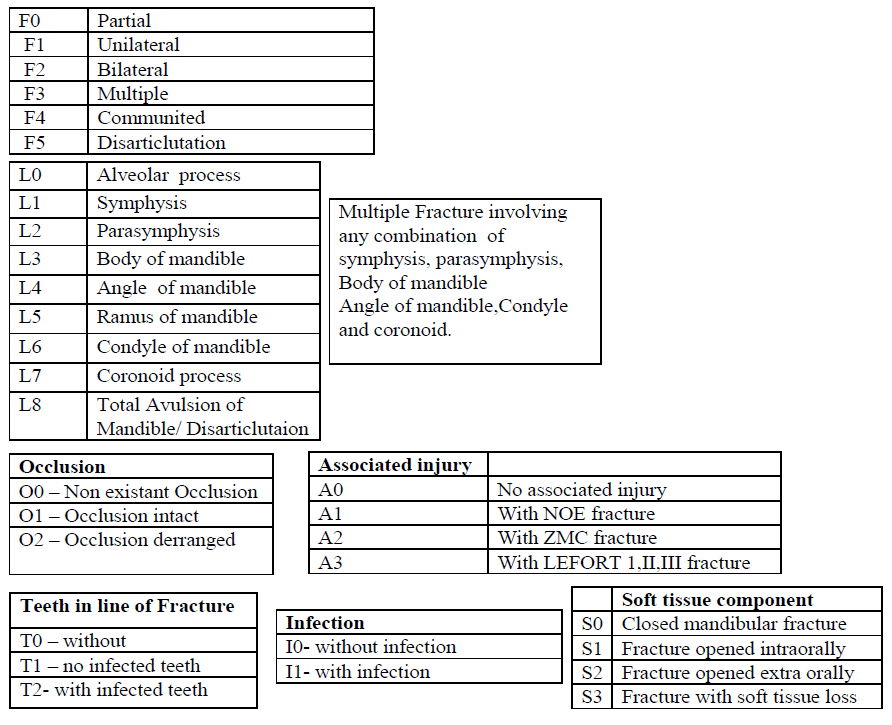
The proposed classification (FLOATIS) almost covers all the required criteria of mandiblar fractures classification like Type of fracture, location and combination of fracture, occlusion, other associated fractures, teeth in line of fracture, presence or absence of infection and soft tissue component. It includes total avulsion of mandible point also into two location i.e., type and site of fracture and exclude the dislocation component. It includes both clinical and radiolographic interpretation of fractures. The demerits of this classification are that it has not included any information related to the primary dentition and also is lengthy.
Passi D & Malkunje L (2017) : Newer proposed FLOATIS classification of mandibular fracture
Conclusion
Fracture is defined as a break or breach in the continuity of normal anatomical structure of a bone by the application of excessive force resulting in two or more fragments of the involved bone. Technically, total avulsion of mandible is not a fracture but is a complete dislocation or disarticulation as a result of maxillofacial trauma. We have discussed various classification systems of mandibular fracture along with their merits and demerits in this review. We proposed a revised classification of mandibular fracture with well-defined categories and its components in a systematic way along with inclusion of unique case of the totally avulsioned mandible in our classification.
Conflict of Interest
All authors disclose that there was no conflict of interest.
REFERENCES
- Hwang K, You SH. Analysis of facial bone fractures: An 11-year study of 2, 094 patients. Indian Journal of Plastic Surgery. 2010;43:42-48.
- Dingman R., Natvig, P. Surgery official fractures, 1969, W. Saunders Company, USA. p. 142-144.
- Kelly D., Harrigan W. A Survey of facial fractures: Bellevue Hospital, 1948-1974. J. Oral Surg., vol.33, Feb., 1975, 145-149.
- Lindahl L, Hollender L. Condylar fractures of the mandible. II. a radiographic study of remodeling processes in the temporomandibular joint. Int J Oral Surg 1977;6:153–165
- Kazanjian VH, Converse JM. Surgical treatment of facial injuries. 3 rd ed. Baltimore: The Williams and Wilkins Company; 1980. p. 66-8.
- Kabakov B., Malishev V. Fractures of jaws, M:Med., 1981; 176.
- Krüger E. Mandibular fractures, 1. Classification, diagnosis and fundamentals of treatment. In: Krüger E, Schilli W. (eds). Oral and maxillofacial traumatology. Chicago: Quintessence Publishing Company; 1982:211–223.
- Sinn D., Hill S, Watson S. Mandibular fractures; In Surgery of facial bone fractures; Foster C., J. Sher-man, Ch. Livingstone, 1987; 171.
- Pogrel MA, Kaban L. Mandibular fracture. In: Habel: Arian BC. Facial fractures, Toronto, Philadelphia. Decker Inc; 1989:183-229.
- Gratz A., In: Inernal fixation of the mandible. B. Spiessl; Springer-Verlag., Berli: Haidelberg, 1989; 375.
- ICD-10 World Health Organization, Geneva, 2003, 261-262.
- Pankratov A., Robustova T. A classification of mandibular fractures. Stomatologia M., 2, 2001, 29-31.
- Shetty V, Atchison K, Der-Matirosian C. The mandible injury severity score: development and validity. J Oral Maxillofac Surg 2007;65:663–670
- Schuknecht B, Graetz K. Radiologic assessment of maxillofacial, mandibular, and skull base trauma. Euro Radio 2005; 15:560-68.
- Buitrago-Téllez CH, Audigé L, Strong B, Gavelin P, Hirsch J, Ehrenfeld M, et al. A Comprehensive Classification of Mandibular Fractures: A preliminary agreement validation study. Inter J Oral Maxillfac Surg 2008; 37:1080-88.
- Passi D, Ram H, Singh G, Malkunje L. Total avulsion of mandible in maxillofacial trauma; Ann Maxillofac Surg. 2014 Jan-Jun; 4: 115–118.



 The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.
The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.