
Vulnerability and Knowledge of Sexually Transmitted Infections Among Female Traders of Reproductive Age in Enugu, Nigeria
- *Corresponding Author:
- Dr. Ikeako LC
Department of Obstetrics and Gynecology, Anambra State University Teaching Hospital, Amaku, Awka, Nigeria.
E-mail: ikeakolawrence@yahoo.com
Abstract
Background: Sexually transmitted infections (STIs) constitute major public health concern and enigma. A comprehensive knowledge of the modes of transmission is necessary to evolve an effective preventive strategy. Aim: The aim of the study is to assess the vulnerability, knowledge and prevention of STIs among female traders of reproductive age in Enugu, Southeast Nigeria. Subjects and Methods: This was a cross‑sectional descriptive study carried out on female traders aged 15‑49 years at Ogbete Main Market, Enugu, Southeast Nigeria. Data was analyzed using Epi‑Info 2000 version 3.3.1 Centers for Disease Control and Prevention Atlanta USA) was used to analyze the data and results were presented in tabular form. Results: A total of 200 female traders of reproductive age participated in the study. The mean (standard deviation) age was 26 (7.4) years. 16% (32/200) were adolescents. Knowledge of specific STIs was highest for human immunodeficiency virus/acquired immune deficiency syndrome 90% (130/200). Parents were poor sources of information as only 28.5% (57/200) respondents heard about STIs from their parents compared with 46% (92/200) from friends and peers. Risk factors identified were multiple sexual partners 75.5% (151/200), non‑use of condoms 62% (124/200) and early debut 58% (116/200). Majority 67.5% (135/200) were aware that STIs could be treated by a visit to the doctor while 21.5% (43/200) preferred traditional/herbal healers. Conclusion: The inclusion of health education in schools’ curricula to ensure that adolescents are adequately aware of STIs, their modes of transmission, prevention and treatment before embarking on any vocation out‑of‑school is advocated.
Keywords
Enugu, Female traders, Knowledge, Prevention, Sexually transmitted infections, Vulnerability
Introduction
Sexually transmitted infections (STIs) are among the most common causes of illness world-wide with far reaching health, public and economic consequences.[1] STIs are a major public health problem due to their serious sequelae when untreated and ability to increase the risk of human immunodeficiency virus (HIV) acquisition and transmission by a factor of 10.[2] Also problematic is the long-term complications, which include pelvic inflammatory disease and cervical cancer.[3] STIs are spread primarily through person-to-person sexual contact.[4]
World-wide, young people under the age of 25 years, who represent nearly half of the world’s population, experience over 100 million new cases of STIs yearly.[4] It is estimated that 80-90% of the global burden of STIs occur in the developing world where there is limited or no access to diagnostics.[4] In general, STIs are more prevalent among African and Caribbean adolescents than in other regions of the world, partly because sexual debut comes as early as 10-11 years in some African and Caribbean countries.[5] A comparative study in Imo State, Nigeria revealed prevalence of 13.9% among post primary schools students aged 11-25 years and 17.16% among tertiary school students aged 16-40 years.[6] This pattern of STIs among adolescents has been attributed to physiologic susceptibility, peer pressure, specific sexual behaviors and lack of access to appropriate treatment.[7].
Apart from the huge costs associated with detection and treatment of STIs, the young men and women infected constituted the work force, especially in developing countries and are thus hindered in their ability to provide for their families and contribute to socio-economic growth of the community.[8] It is estimated that STIs account for 17% of economic losses due to ill health in developing countries[9] while in America, the life time medical costs of STIs acquired by youth ages 15-24 in the year 2000 were estimated at 6.5 billion dollars.[8]
Most studies on the knowledge and awareness of STIs in this area concentrated on schools[5] and adolescents usually categorized as vulnerable.[2,7] There are various interest groups and the extent of knowledge and awareness vary.
In view of this, this present study was conducted among female traders of reproductive age in Enugu, Southeast Nigeria to assess their vulnerability and knowledge of STIs and its prevention. The outcome could be used for planning interventions for prevention and control of STIs.
Subjects and Methods
The study was conducted on female traders of reproductive age (15-49 years) in Ogbete Main Market (OMM) Enugu, in March 2009.
OMM is located Enugu North Local Government Area of Enugu State, Southeast Nigeria. It has a land mass of about 600 m2 and about 12,000 traders. OMM was purposefully chosen out of the three major markets in Enugu because it is the largest and therefore the most representative of female traders of reproductive age.
A descriptive cross-sectional study design was used.
Approval for this study was obtained from the Ethical Committee of University of Nigeria Teaching Hospital, Enugu and informed verbal consent from the respondents. For the minors, consent was obtained from either their parents or guardians.
The sample size was calculated using the formula below for estimated population size of less than 10,000.[10]
N = Z2 P (1-p)/D2
Where N = minimum sample size;
Z = 1.96 at 95% confident limit;
D = margin of error tolerated = 5%;
p = prevalence of knowledge of STIs;
N = 1.962 × 87.7 (100-87.7)/52 = 166;
Minimum sample size = 166.
Adding 20% of the minimum sample size for the expected non-response rate, a sample size of 200 was obtained.
By simple random sampling method, four sections (food stuff, provisions, cosmetics and clothing/fashion) out of the seven sections (others are books/stationery, electronics and drugs) in the market were selected.
The sample size of 200 was divided equally among the four selected sections, resulting to 50 respondents from each section. Each of the selected sections has between 3 and 4 rows, alphabetically numbered in line with the section numbering of the market. Each selected section was visited and from one end of a row, shops were consecutively selected and women of reproductive age met in each shop, who gave informed consent, were interviewed. Any shop without women of reproductive age was skipped and the next in that row was selected. The same procedure was adopted row after row until the sample size of 50 respondents for that section was interviewed.
Hawkers and sellers without designated shops were excluded from the study.
Data was collected using a pre-tested interviewer-administered questionnaire with open and closed ended questions. The questionnaire was made up of four sections; section (A) included socio-demographic data, (B) knowledge of the causes of STIs, (C) knowledge of prevention of STIs and (D) knowledge of vulnerability/risk factors for STIs.
Data was analyzed using Epi-info version 3.3.1 (Centers for Disease Control and Prevention Atlanta, Georgia, USA) and results were presented in tabular form.
Results
A total of 200 female traders of reproductive age participated in the study. Table 1 shows the socio-demographic characteristics of the respondents.
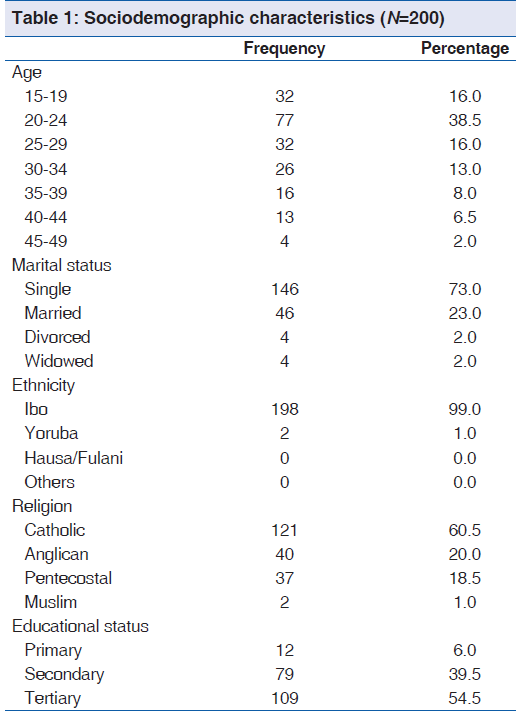
The mean (standard deviation) age was 26 (7.4) years. Nearly, 16% (32/200) were adolescents. Majority 73% (146/200) were single and had secondary education 39.5% (79/200).
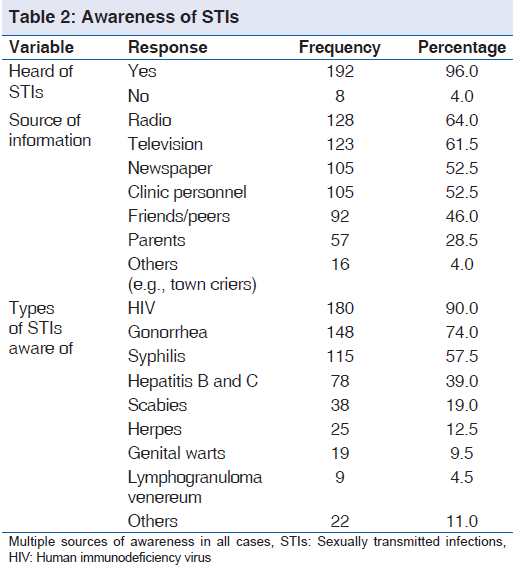
Table 2 shows the respondents’ awareness of STIs. The most common source of information was radio 64% (128/200) and knowledge of specific STIs was highest for HIV 90% (180/200). Majority 83% (166/200) knew that STIs can be acquired through unprotected sexual intercourse.
The symptoms of STIs as identified by the respondents were vaginal discharge 56% (112/200), ulcers 24% (49/200), vulva itching 39.5% (79/200) and abdominal pain 34% (68/200). Others were weight loss 51.5% (103/200), painful micturition 47.5% (95/200) and diarrhea 23.5% (47/200).
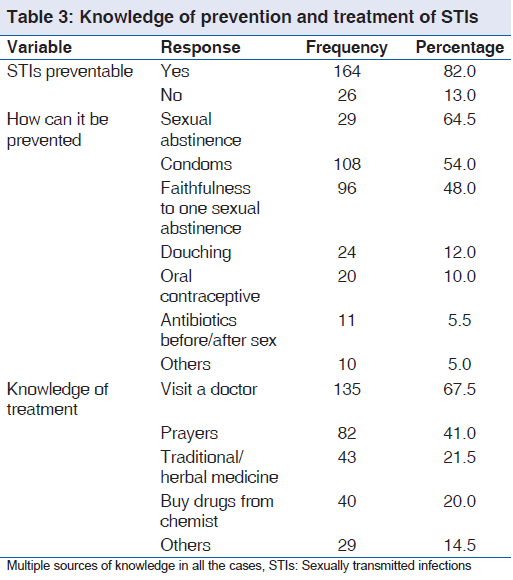
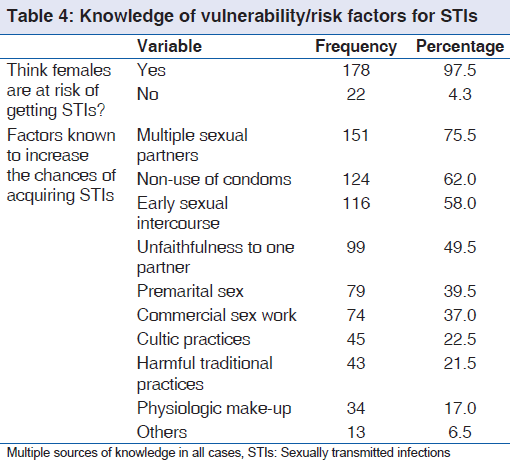
The knowledge of prevention and treatment of STIs is shown in Table 3. Sexual abstinence 64.5% (129/200) and visiting a doctor 67.5% (135/200) were the preferred methods of prevention and treatment respectively. Table 4 shows knowledge of vulnerability/risk factors for STIs. Majority 95.7% (178/200) cited that females were at risk of getting STIs and the most common reason given for this vulnerability was having multiple sexual partners 75.5% (151/200).
Discussion
The study was carried out on 200 female traders aged 15-49 years drawn from four of the seven major section of OMM. 16% (32/200) were adolescents and these may be the most exposed to dangers of prevalent STIs given their naivety and lack of assertive skills.[11]
Around 90% (180/200), 74% (148/200) and 57.5% (115/200) of the respondents had heard about HIV/acquired immune deficiency syndrome (AIDS), gonorrhea and syphilis respectively. Other studies reported low levels of awareness of STIs, with the exception of HIV/AIDS.[12,13] A study in Bangladesh revealed that 45.2% of the participants did not hear the name of AIDS.[14]
The high level of awareness in this study may be due to the health education provision by Nigeria’s HIV/AIDS control program (National Action Committee on AIDS) through radio jingles, print and electronic media. Enugu is an urban area with efficient means of dissemination of such information. In a similar study in rural Delta State Nigeria, only 13.1% of the participants had knowledge of STIs.[15] It was concluded that this could be related to the peculiarities of the rural areas where means of disseminating information may not be as efficient as in the urban.[15]
The study reiterates the fact that parents are poor sources of information as only 28.5% (57/200) of the respondents heard about STIs from their parents as compared with 46% (92/200) who got the information from friends/peers. In Dares Salaam, it was reported that a relatively low proportion of parents were willing to talk to their children on sex related issues, preferring that such issues should be taught at schools.[16] The poor parental contribution to source of information on STIs could be attributed to lack of knowledge on sexual and reproductive matters and the belief that such discussions “corrupt” young people and encourage early experimentation.[17,18]
Unprotected sexual intercourse and vaginal discharge were the most common mode of transmission and symptom known by the respondents. This is in line with other reports.[19,20]
The participant identified the following risk behaviors; multiple sexual partners 75.5% (151/200), non-use of condom 62% (124/200), early sexual debut 58% (116/2000) and pre-marital sex 39.5% (79/200). These have been reported in other studies.[5,20,21] Most women regard condoms primarily as a method of contraception and not as a means of protection against STIs.[17] A good number of the respondents 82% (164/200) knew that STIs are preventable and while 64.5% (120/200) said that it can be prevented by sexual abstinence, 54% (108/200) believed condom use can be preventive. Other measures thought to prevent STIs are douching after sex 12% (24/200), oral contraceptive 10% (20/200) and antibiotics before and after sex 5.5% (11/200). This is different from a previous study in which as much as half of the respondents believed that the use of antibiotics before sex could protect from STIs while only 27.2% reported that condom use could be protective.[22] The difference is probably due to improved publicity on the mode of transmission and prevention of HIV/AIDS and the advertisement of different makes of male condoms. On modes of treatment of STIs, 67.5% (135/200) knew that visit to the doctor is necessary while 41% (82/100) and 21.5% (43/200) resorted to prayers and traditional/herbal healers respectively. The use of the informal sources for treatment could be attributed to the greater accessibility, low cost, convenience, confidentiality, less judgmental and less stigmatizing nature of the services.[23]
The limitations of the present study should be acknowledged along with the directions for future research. The findings of this study cannot be generalized to the whole population of women because of the small sample size. Another limitation is that the study did not investigate the association between the variables analyzed. Also, we assessed the knowledge using closed ended questions, which have an inherent weakness of guesswork.[24] It cannot be ruled out that some participants, unable to answer the question, selected answers at random. In future studies, it would be interesting to examine whether the use of open-ended questions leads to similar findings.
The majority of the market women in the study heard about STIs from electronic and print media while parents were poor sources of information. There is a need to articulate program, which include messages aimed at reinforcing safer sex practices for women who are already sexually active. The inclusion of health education in schools’ curricula to ensure that adolescents are adequately aware of STIs, their modes of transmission, prevention and treatment before embarking on any vocation out of school is advocated.
Since poverty limits the decision making ability and reduces the safe sex negotiating skills of women,[25] efforts at achieving the millennium development goal of eradicating extreme poverty and hunger should be intensified.
Source of Support
Nil.
Conflict of Interest
None declared.
References
- DiClemente RJ, Salazar LF, Crosby RA. A review of STD/HIV preventive interventions for adolescents: Sustaining effects using an ecological approach. J Pediatr Psychol 2007;32:888-906.
- Mmari KN, Oseni O, Fatusi AO. STI treatment-seeking behaviors among youth in Nigeria: Are there gender differences? Int Perspect Sex Reprod Health 2010;36:72-9.
- Ohene S, Akoto I. Factors associated with sexually transmitted infections among young Ghanaian women. Ghana Med J 2008;42:96-100.
- WHO (World Health Organization). Global Strategy for the Prevention and Control of Sexually Transmitted Infections: 2006-2015. Geneva: WHO; 2007. Available from: http://www. who.int/reproductive health/publications/stisstrategy/ pdf. [Retrieved on 2009 Apr 12].
- Chinsembu KC, Siziya S, Muula AS, Rudatsikira E. Prevalence and social correlates of sexual intercourse among school-going adolescents in Namibia. Sahara J 2008;5:129-35.
- Obiajuru OC, Jude NO. The prevalence of sexually transmitted infections among post primary and tertiary school students in Imo state, Nigeria. Niger J Health Bio Sci 2007;6:90-5.
- Okereke CI. Sexually transmitted infections among adolescents in a rural Nigeria. Indian J Soc Sci Res 2010;7:32-40.
- Chesson HW, Blandford JM, Gift TL, Tao G, Irwin KL. The estimated direct medical cost of sexually transmitted diseases among American youth, 2000. Perspect Sex Reprod Health 2004;36:11-9.
- Mayaud P, Mabey D. Approaches to the control of sexually transmitted infections in developing countries: Old problems and modern challenges. Sex Transm Infect 2004;80:174-82.
- Margret AO. Research Methodology with Statistics for Health and Social Sciences. 1st ed. Ilorin, Nigeria: Nathader Publishers; 2003:115-21.
- Esere MO. Effect of sex education programme on at-risk sexual behaviour of school-going adolescents in Ilorin, Nigeria. Afr Health Sci 2008;8:120-5.
- Samkange-Zeeb FN, Spallek L, Zeeb H. Awareness and knowledge of sexually transmitted diseases (STDs) among school-going adolescents in Europe: A systematic review of published literature. BMC Public Health 2011;11:727.
- Fageeh WM. Awareness of sexually transmitted diseases among adolscents in Saudi Arabia. JKAU Med Sci 2008;15:77-90.
- Rahman MM, Kabir M, Shahidullah M. Adolescent knowledge and awareness about AIDS/HIV and factors affecting them in Bangladesh. J Ayub Med Coll Abbottabad 2009;21:3-6.
- Ogbe JO. Knowledge, sources of information and practice of condom use in the prevention of sexually transmitted infections (STIs) among rural dwellers in Delta State, Nigeria. Ethno Med 2011;5:107-14.
- Tengia-Kessy A, Kamugisha H. Levels of knowledge and sources of information on sexually transmitted infections among secondary school youth in Dar ES Salaam, Tanzania. East Afr J Public Health 2006;3:19-22.
- Bastien S, Kajula LJ, Muhwezi WW. A review of studies of parent-child communication about sexuality and HIV/AIDS in sub-Saharan Africa. Reprod Health 2011;8:25.
- Mbugua N. Factors inhibiting educated mothers in Kenya from giving meaningful sex-education to their daughters. Soc Sci Med 2007;64:1079-89.
- Sri Devi B, Swaranalatha N. Prevalence of RTI/STI among reproductive age women (15-49 years) urban slums of Tirupati town, Andhra Pradesh. Health Popul Perspect Issues 2007;30:56-70.
- Aboyeji AP, Adeggoke AA, Adebisi SA. Sexual behaviour and knowledge of sexually transmitted diseases among female adolescents in Ilorin, Kwara State, Nigeria. Trop J Med Res 2004;8:10-5.
- Mutinta G, Govender K, Gow J. George G. An exploratory study of the individual determinants of students’ sexual risk behavior at a South African University. Afr J AIDS Res 2012;11:353-9.
- Sunmola AM, Dipeolu M, Babalola S, Adebayo OD. Reproductive knowledge, sexual behaviour and contraceptive use among adolescents in Niger State of Nigeria. Afr J Reprod Health 2003;7:37-48.
- Dehne K, Riedner G. Sexually Transmitted Infections among Adolescents: The Need for Adequate Health Services. Geneva: WHO; 2005.
- Krause N. A comprehensive strategy for developing closed-ended survey items for use in studies of older adults. J Gerontol B Psychol Sci Soc Sci 2002;57:S263-74.
- Salazar LF, Crosby RA, DiClemente RJ, Wingood GM, Lescano CM, Brown LK, et al. Self-esteem and theoretical mediators of safer sex among African American female adolescents: Implications for sexual risk reduction interventions. Health Educ Behav 2005;32:413-27.



 The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.
The Annals of Medical and Health Sciences Research is a monthly multidisciplinary medical journal.